





The Number That Should Alarm Everyone in Healthcare
In May 2026, the American Association of Colleges of Nursing released its annual enrollment survey. Buried in the data was a number that should have made national news but barely registered outside of academic nursing circles:
U.S. nursing schools turned away 93,176 applications.
Not unqualified applicants. Not students who didn’t meet the GPA requirements or failed the prerequisite coursework. Qualified applicants, people who met every admission standard and were still told no.a
To put that in perspective: 93,176 is larger than the entire population of cities like Green Bay, Wisconsin or Bend, Oregon. It’s more people than the U.S. Army recruited in all of 2024. It’s enough qualified, motivated individuals to staff the nursing departments of hundreds of hospitals — if only someone could train them.
And the trendline is accelerating. Here’s what the last five years look like:
2021: 91,938 qualified applications turned away
2022: 78,191 qualified applications turned away
2023: 65,766 qualified applications turned away
2024: 80,162 qualified applications turned away
2025: 93,176 qualified applications turned away
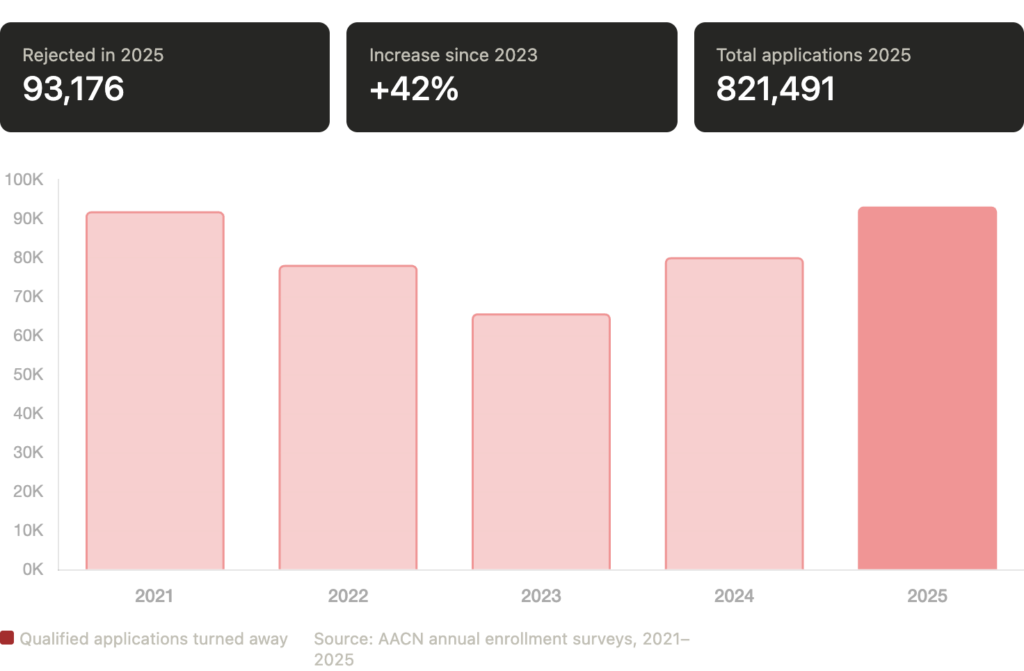
After dipping during the post-pandemic enrollment slump, rejections have surged back to record levels, driven by an application boom that the system simply cannot absorb. Total applications to baccalaureate and higher degree nursing programs reached 821,491 in 2025, an increase of 92,672 from the prior year. More people want to become nurses than at any point in American history.
The pipeline isn’t failing because of a lack of interest. It’s failing because it can’t hold the volume.
Where the Rejections Are Happening
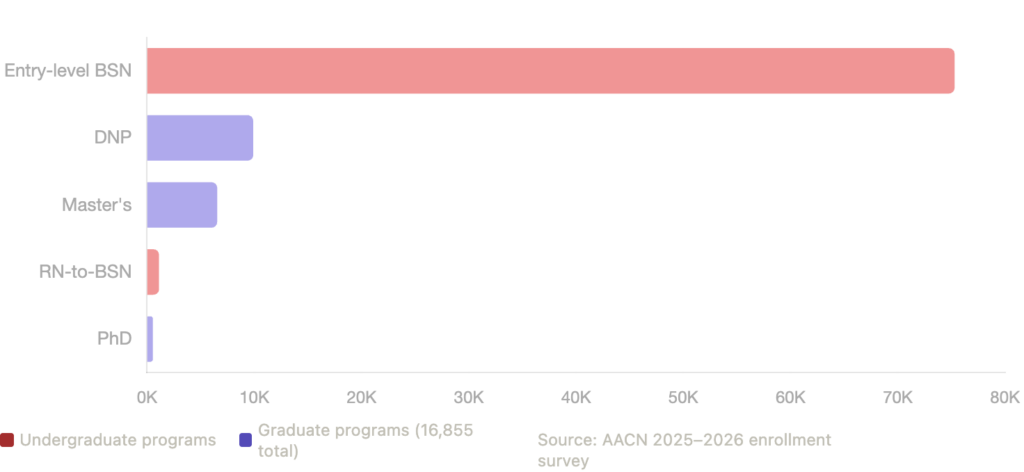
The 93,176 rejections don’t fall evenly. Breaking them down reveals where the pipeline is most constrained:
Entry-level baccalaureate (BSN) programs accounted for 75,255 of the rejected applications, roughly 81% of the total. These are prospective nurses trying to enter the profession for the first time. When we talk about the nursing workforce pipeline, this is the widest part of the funnel, and it’s the most clogged.
DNP programs saw 9,859 applications turned away, the highest graduate-level rejection total in the dataset. Doctor of Nursing Practice programs produce the advanced practice nurses (NPs, CNSs, nurse anesthetists) that the workforce desperately needs, particularly in primary care, psychiatry, and rural health.
Master’s programs turned away 6,496 applications. Combined with DNP rejections, that’s nearly 17,000 applications rejected from graduate programs alone, a number AACN flagged with particular concern because these are the programs that produce nurse educators, and without more educators, the cycle of constrained capacity perpetuates itself.
PhD programs rejected 500 applications. That number may sound small in comparison, but context matters: PhD enrollment has declined for eleven consecutive years, falling 20.8% since 2013. The total number of PhD nursing students in the U.S. is now just 4,077. Every rejected PhD application represents a potential nursing researcher, scientist, or faculty member that the system will never produce.
The Five Barriers — And Why They’re Getting Worse, Not Better
AACN’s survey is consistent in identifying the same barriers year after year: insufficient clinical placement sites, budget constraints, a shortage of faculty, a shortage of preceptors, and insufficient classroom space. But understanding why these barriers are intensifying despite widespread awareness that they exist requires looking at each one individually.
Barrier 1: Clinical placement sites.
Every nursing student must complete supervised clinical hours in healthcare settings; hospitals, clinics, community health centers, long-term care facilities. These placements require formal agreements between schools and clinical partners, and the number of available slots is finite. As programs grow and new schools open, they’re all competing for the same pool of clinical sites, often in the same metropolitan areas. Rural programs face the opposite problem: there simply aren’t enough clinical settings within driving distance to accommodate their students.
The clinical placement bottleneck is the single most frequently cited barrier to expansion, and it’s the one that traditional solutions, building more classrooms, hiring more faculty, cannot address on their own. You can double a program’s lecture hall capacity overnight. You cannot double the number of hospitals willing to take your students.
Barrier 2: Faculty shortages.
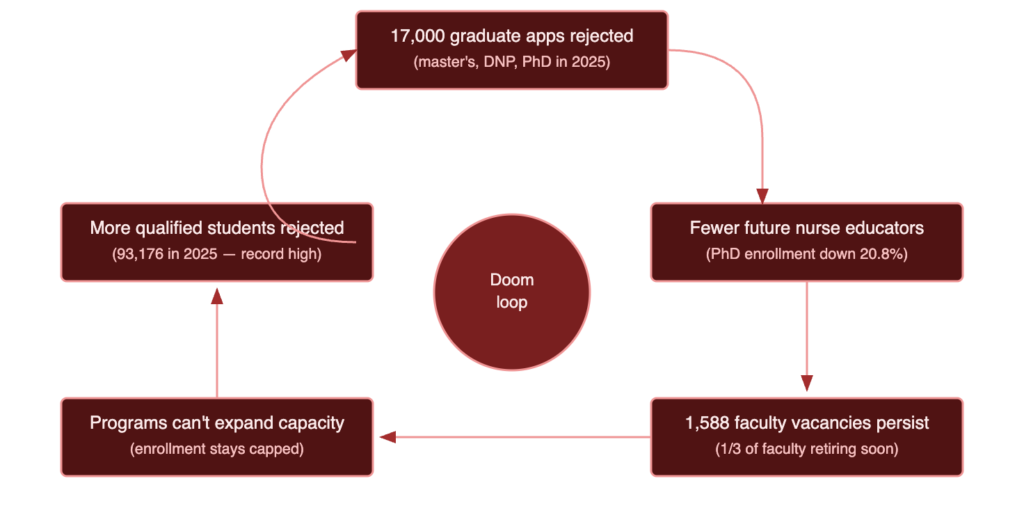
Nursing schools reported 1,588 full-time faculty vacancies in the most recent survey. One-third of current nursing faculty are expected to retire within the next decade. And the reason replacements aren’t lining up is straightforward: nursing faculty salaries are 20-30% lower than what the same individual could earn in clinical practice. A nurse practitioner earning $130,000 in clinical care has little financial incentive to take a faculty position paying $95,000, especially when that position requires a terminal degree that took years to complete.
This creates a doom loop. Fewer faculty means fewer students admitted. Fewer students in graduate programs means fewer potential future faculty. Graduate applications getting rejected (17,000 in 2025) further shrinks the pipeline of people who could eventually become educators. The system is cannibalizing its own future.
Barrier 3: Preceptor availability.
Clinical preceptors — the licensed providers who supervise nursing students during their clinical hours are overwhelmingly unpaid. Ninety percent of U.S. nursing programs do not compensate their preceptors. The providers who do choose to precept are volunteering their time and absorbing slower patient throughput, all while managing their own clinical workloads. It’s no surprise that a significant percentage report burnout from precepting, with nearly half citing negative impacts on their personal and professional lives.
When preceptors burn out and stop volunteering, programs lose placements. When programs lose placements, they can’t admit as many students. The preceptor shortage doesn’t make headlines the way hospital staffing shortages do, but it’s arguably more consequential because it constrains the supply of every future nurse, NP, and clinical leader.
Barrier 4: Budget constraints.
State funding for public universities has been flat or declining in real terms for decades. Federal support for nursing education, while significant, hasn’t kept pace with enrollment demand. AACN has specifically warned that current efforts to curtail federal support for nursing schools and graduate education could reverse the positive enrollment trends observed in 2024-2025. Programs that can’t fund new faculty lines, clinical simulation equipment, or expanded partnerships are stuck at their current capacity, regardless of how many qualified applicants knock on the door.
Barrier 5: Classroom and lab space.
This is the most straightforward constraint and the least interesting to write about, but it’s real. Nursing programs require specialized lab spaces for simulation, skills practice, and testing. These facilities are expensive to build and maintain, and many schools, particularly those housed in older university buildings have maxed out their physical footprint. Online and hybrid programs have partially addressed this through distance learning for didactic coursework, but clinical simulation and skills labs still require physical presence.
The Compounding Problem No One Is Talking About
There’s a secondary crisis embedded in the 93,000 number that deserves its own spotlight: the graduate rejection pipeline.
Of the 93,176 total rejections, nearly 17,000 came from graduate programs; master’s, DNP, and PhD. These aren’t entry-level nursing candidates. These are working nurses seeking to advance into nurse practitioner roles, clinical leadership, education, and research.
This matters for three specific reasons.
First, NPs are the fastest-growing segment of the healthcare workforce. The Bureau of Labor Statistics projects 40% employment growth for nurse practitioners between 2023 and 2033. Every rejected DNP or master’s application is a delayed or lost NP — a provider who won’t be available to see patients in underserved communities, staff rural clinics, or reduce the physician workload that’s driving burnout across the system.
Second, nursing faculty positions overwhelmingly require a master’s or doctoral degree. When 17,000 graduate applications are rejected, the pool of potential future faculty shrinks. This means the faculty shortage that’s already constraining undergraduate admissions will get worse, not better. We’re rejecting the people who could solve the rejection problem.
Third, PhD enrollment has declined for eleven consecutive years. The 20.8% drop since 2013 means the nursing profession is producing fewer researchers, fewer scientists, and fewer academic leaders every year. At just 4,077 total PhD nursing students nationwide, the program that trains the profession’s future is itself in decline.
This is what a compounding crisis looks like: the system’s inability to train enough nurses today is directly undermining its ability to train nurses tomorrow.
What Has to Change
The 93,000 number will get worse before it gets better — unless the constraints that drive it are addressed structurally, not incrementally. Here’s what that requires.
Expand clinical placement capacity through technology. The most binding constraint — clinical site availability — cannot be solved by building more hospitals or convincing more clinics to sign affiliation agreements. Virtual clinical education platforms can connect nursing students to supervised telehealth precepting experiences that don’t compete for the same physical slots as traditional rotations. CMS permanently approved virtual supervision for teaching physicians in January 2026, removing the regulatory ambiguity that previously limited adoption. Programs that integrate virtual placements alongside in-person rotations can expand their total clinical capacity without being limited by local site availability.
Invest in the preceptor workforce. The expectation that experienced clinicians will supervise students for free is a model that has reached its breaking point. Six states have enacted preceptor tax credits, and the bipartisan PRECEPT Nurses Act would create the first federal incentive. But financial recognition alone isn’t sufficient — the precepting model itself needs to become less burdensome. Virtual precepting platforms reduce the time cost of supervision by integrating teaching into existing telehealth encounters rather than adding it on top of in-person clinical workloads.
Fund faculty salaries at competitive levels. The Nurse Faculty Shortage Reduction Act, a bipartisan bill introduced in both the House and Senate, would create a federal program to supplement nursing educator salaries and help schools recruit and retain faculty. Until the 20-30% salary gap between clinical practice and academia is closed, the profession will continue to lose its best educators to the bedside. This isn’t a criticism of clinical nursing, it’s an acknowledgment that the market incentives are misaligned, and policy intervention is needed.
Protect federal support for nursing education. AACN has explicitly warned that current proposals to curtail federal funding for nursing schools and graduate education could reverse the enrollment gains of 2024-2025. At the exact moment when applications are surging and the workforce need is most acute, reducing support for the institutions that train nurses would be the policy equivalent of turning off a fire hydrant during a fire.
Treat clinical education capacity as a national workforce metric. Every state tracks healthcare workforce shortages. Almost none track clinical education capacity as a leading indicator. If 93,000 rejected applications in 2025 predict a provider shortage in 2035, why isn’t training capacity measured, reported, and invested in with the same urgency as hospital staffing ratios?
The Bottom Line
93,176 is not just a data point. It’s a policy failure, an infrastructure failure, and a moral failure. Every one of those rejected applications represents a person who wanted to become a nurse, who met the qualifications, did the work, and was told the system doesn’t have room for them.
And the cruelest irony is this: we will spend the next decade talking about the nursing shortage — about hospitals that can’t fill positions, about patients who can’t access care, about rural communities that lose their last provider — while simultaneously turning away the very people who volunteered to solve it.
The demand is there. The students are there. What’s missing is the infrastructure to train them.
93,176 qualified applications rejected. Not because the students weren’t good enough. Because the pipeline wasn’t big enough.
That’s the breaking point. And we’ve reached it.
MomentMD is building the clinical education infrastructure to help close this gap. With 50+ university partnerships, over 300,000 clinical hours delivered, and a nationwide network of board-certified preceptors, MomentMD helps nursing and graduate health programs expand placement capacity, guarantee rotations, and admit more of the students who are ready to serve. Learn how we can help your program.